Many a time you come across the patients presented with history of haemoptysis in ur clinical practises.It is defined as expectoration of blood, or bloody sputum. Haemoptysis is common. In most cases, it is mild, self-limiting and related to transitory infection but it should be considered a serious sign due to the risk of underlying pathology. The relative contribution of different causes depends on the local population.
Defintion Haemoptysis is the coughing of blood originating from the respiratory tract below the level of the larynx. Haemoptysis should be differentiated from:
- Haematemesis - vomiting of blood from the gastrointestinal (GI) tract.
- Pseudohaemoptysis - where a cough reflex is stimulated by blood not derived from the lungs or bronchial tubes. This may be from the oral cavity or nasopharynx (eg following an epistaxis) or following aspiration of haematemesis into the lungs.
Types of Haemoptysis:
- Frank haemoptysis It is the expectoration of blood only. Massive and fatal blood loss may occur. Frank haemoptysis daily suggests bronchogenic carcinoma.
- Haemoptysis in suppurative lung disease Large quantities of foul smelling sputum and blood suggests suppurative lung disease.
- Spurious haemoptysis Haemoptysis present secondary to upper respiratory tract infection, above the level of larynx.
- Pseudohaemoptysis It is due to pigment, prodigiosin produced by gram-negative organism, Serratia marcescens.
- Endemic haemoptysis Present in infection with Paragonimus westermani (lung fluke).
Severity of Haemoptysis:
Blood loss volume is more useful in guiding management than determining diagnosis although bleeding from the low pressure, pulmonary system tends to be small volume whilst that from the bronchial system, which is at systemic pressure, tends to be more profuse.
- Mild: less than 100 ml blood loss per day
- Moderate: 100–150 ml blood loss per day
- Severe :Up to 200 ml blood loss per day
- Massive :Greater than 500 ml blood loss per day (or) rate of blood loss greater than 150 ml/hr (or) 100 ml blood loss per day for more than 3 days.
Causes of Haemoptysis:
There a number of pathological causes that can present with Haemoptysis.Some of the common causes are listed below.But a definitive diagnosis require several other investigations.
Infection:
a. Tuberculosis
b. Lung abscess
c. Bronchiectasis
d. Pneumonia
e. Fungal infection (aspergillosis, nocardiosis, blastomycosis).
Neoplasm:
a. Bronchogenic carcinoma
b. Bronchial adenoma
c. Metastatic tumour to lung.
Cardiovascular Disorders
a. Mitral stenosis
b. Pulmonary hypertension
c. Aortic aneurysm
d. Arteriovenous malformation
e. Pulmonary embolism
.Congenital
a. Bronchial cyst
b. Sequestration of lung
i. Intralobar
ii. Extralobar
Collagen Vascular Disorder
a. Vasculitis
b. Wegener’s granulomatosis
c. Goodpasture’s syndrome.
Traumatic
a. Non-iatrogenic
i. Blunt injury
ii. Inhalation of toxic gases or acid aspiration
b. Iatrogenic
i. Diagnostic: Biopsy procedure
ii. Therapeutic: Anticoagulants,Radiation fibrosis.
Miscellaneous
Bleeding disorders.
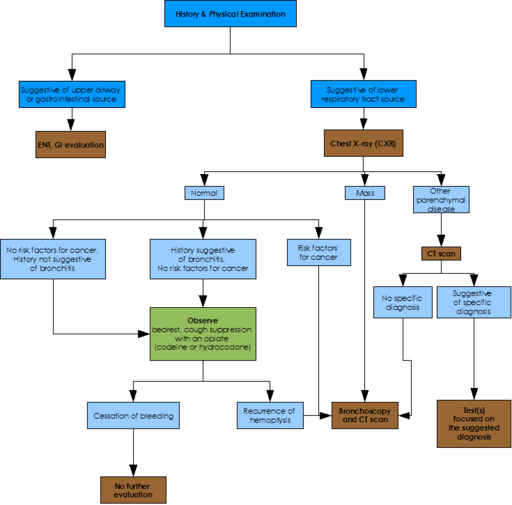
Diagnostic approach to a case of Haemoptysis:
Since Haemoptysis is a very common clinical presentation of various diseases. The diagnostic approach therefor include taking an appropriate clinical history,physical examination and proper and reliable investigations.
- Past history, History of present illness, Family history: History of tuberculosis, Bronchiectasis, chronic bronchitis, mitral stenosis, etc. History of smoking, occupational diseases by exposure to silica dust, etc.
- Blood Duration, Frequency, Amount Amounts of blood: large amounts of blood, or is there blood-streaked sputum Probable source of bleeding: Is the blood coughed up, or vomited?
- Bloody sputum Color, characters: blood-streaked, fresh blood, frothy pink, bloody gelatinous.
- Accompanying symptoms Fever, chest pain, coughing, purulent sputum, mucocutaneous bleeding, jaundice.
- Imaging examination Chest X-ray, CT scan and 3D reconstruction images or CT virtual bronchoscopy, bronchial angiography.
- Laboratory tests Blood test: WBC Sputum: cells and bacterial examinations, sputum culture
- Bronchial fiber endoscopy

Mangement
With a proper history and investigations we can arrive to proper diagnosis of the underlying cause.Treatment depends largely upon the underlying cause. Many modalities of treatment can be used, like, iced saline, or topical vasoconstrictors, such as adrenalin or vasopressin can be used. Selective bronchial intubation can be used to collapse lung in which the hemorrhage is occurring, also endobronchial tamponade can be used. Laser photocoagulation can be used to stop bleeding during bronchoscopy. Angiography of bronchial arteries can be performed to locate the bleeding, and it can often be embolized. Surgical option is usually the last resort, and can involve, lobectomy or pneumonectomy
No comments:
Post a Comment